Nicole Boynosky, BVMS, MS, DACVD
Veterinary Specialty Hospital, San Diego, CA
Posted on 2017-05-09 in Dermatology
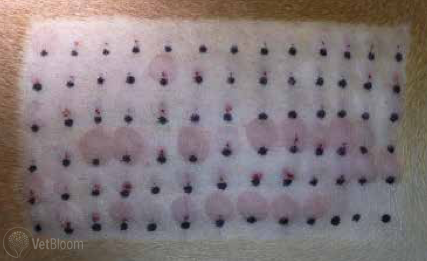
Intradermal skin test of a 4-year-old pit bull terrier. Note the multiple positive erythematous reactions.
Atopic dermatitis (AD) is a complicated multifactorial disease that includes epidermal barrier dysfunction, IgE-mediated hypersensitivity, environmental and epigenetic factors, environmental allergens, diet-induced AD, and immune dysregulation. Currently, many different treatment options are available, some of which are more successful than others. Allergen-specific immunotherapy (ASIT) is the only therapy that has the potential to change the immunologic response to allergens. AD is a diagnosis of exclusion, therefore before performing serum or intradermal skin testing, we must diligently identify all potential causes of pruritus, rule out other types of allergy, and ensure that the diagnostic criteria for AD are fulfilled. The first step in diagnosis involves identifying and managing infectious causes pruritus (i.e., bacterial and fungal) and ruling out ectoparasites (i.e., Sarcoptes and fleas). Year-round flea prevention is paramount; the presence of fleas, particularly if the patient has a documented hypersensitivity to flea bites/saliva, can be a major contributing factor to pruritus. Without a strong seasonal history of clinical signs that cannot be attributed to flea saliva, the second essential step is to pursue a prescription-based novel or hydrolyzed diet elimination trial to rule out any component of cutaneous adverse food reactions (CAFR). The duration of the diet trial typically ranges from 8 to12 weeks, although 10- to 12-week trials may be necessary, particularly if the patient’s skin has been damaged by chronic inflammation and pruritus. Understanding the role of diet in the patient’s pruritus is critical, especially in non-seasonal San Diego, as it can greatly affect the success of the ASIT. When all is said and done, appropriate diagnosis of AD can take months.
AD was defined by Dr. Halliwell as a ‘genetically predisposed inflammatory and pruritic skin disease with characteristic features, it is associated most commonly with IgE antibodies to environmental allergens.’ AD is more likely if patients exhibit 5 or more of Favrot’s criteria: age of onset less than 3 years (typically 1-3 years), chronic recurrent Malassezia infections, housed indoors, glucocorticoid responsive, affected front paws, affected concave pinna, no involvement of pinnal margins (if affected, highly suspect scabies), nonaffected dorsolumbar trunk (if affected, suspect flea component).
Once potential exposure to ectoparasites has been addressed, the role of diet has been evaluated and managed, and Favrot’s criteria have been fulfilled, then testing for environmental allergens is indicated. As mentioned, AD is a diagnosis of exclusion, allergy testing does not provide a diagnosis for AD. Healthy dogs without AD can show multiple strong positives on skin and serum testing. Testing is employed with the expectation of subsequent desensitization/hyposensitization, as it is unrealistic to expect to keep our patients isolated from the various aeroallergens. These tests are diagnostic aids used to determine allergens for inclusion for the desensitization serum. Use of serum allergy testing and/or intradermal skin testing (IDST) is completely inaccurate for testing for diet allergens and it is widely accepted that a diet trial is the only means to diagnose CAFR.
IDST is considered the gold standard, however, some patients (i.e., those with severe and persistent dermatologic lesions, infections, or patients with chronic urticaria) are not always ideal candidates and serum testing may be employed. Not all serum allergy tests are created equal and choosing the wrong one may affect the results greatly. Determination of which allergens to include in the desensitization serum and the protocol used are critical aspects of this process. Although the mechanism of ASIT is not completely understood, one aspect is the production of “blocking” allergen-specific IgG antibodies produce increasing the production of allergen-specific IgG as opposed to IgE. Recent studies in humans have also shown that IDST changes the immune response upon allergen exposure towards allergen-specific T-regulatory cells and away from allergen-specific Th1 and Th2, therefore decreasing the pro-inflammatory that they induce. Mast cell and eosinophil tissue infiltration is also decreased.
Extensive client discussion and an extensive dermatologic workup are important prior to testing. Therapy must be customized to the individual dog. The needs of the owner and the test results influence the desensitization method used (i.e. subcutaneous injections vs allergen-specific immunotherapy). Most of the literature supports a 60% to 75% success rate when used in the correct context. Success is often higher when therapy is adjusted based on patient response. The younger the dog is when AD is diagnosed and ASIT is started, the higher the success rate. There is an art to managing these dogs, and treatment often requires much more than ASIT alone, particularly during the initial phase of therapy. Results may not become apparent for anywhere from a few months to 18-24 months.
About the author
|
 Dr. Nicole Boynosky is originally from Pennsylvania, where she obtained a Master’s degree in Laboratory Animal Science from Drexel University in Philadelphia. She crossed the Atlantic and lived in Scotland for 5 years, graduating with distinguished honors from the University of Glasgow in 2007. Dr. Boynosky practiced general medicine in Cherry Hill New Jersey from 2007 to 2010. She then moved to sunny southern California, where she completed a specialty internship in veterinary dermatology followed by a three-year dermatology residency at Veterinary Specialty Hospital under the mentorship of Dr. Laura Stokking. Dr. Boynosky is interested in all aspects of dermatology, but has particular interests in immune-meditated disease, multi-drug resistant bacterial infections, and allergy. Dr. Boynosky enjoys teaching staff, students, and other veterinarians about dermatology and has several publications in the field of dermatology and clinical microbiology. When she is not at VSH, she enjoys spending time with her retired racing Greyhound turned couch potato named Jack, and her very huggable and cuddly rescued Pit bull named Hadley.
Dr. Nicole Boynosky is originally from Pennsylvania, where she obtained a Master’s degree in Laboratory Animal Science from Drexel University in Philadelphia. She crossed the Atlantic and lived in Scotland for 5 years, graduating with distinguished honors from the University of Glasgow in 2007. Dr. Boynosky practiced general medicine in Cherry Hill New Jersey from 2007 to 2010. She then moved to sunny southern California, where she completed a specialty internship in veterinary dermatology followed by a three-year dermatology residency at Veterinary Specialty Hospital under the mentorship of Dr. Laura Stokking. Dr. Boynosky is interested in all aspects of dermatology, but has particular interests in immune-meditated disease, multi-drug resistant bacterial infections, and allergy. Dr. Boynosky enjoys teaching staff, students, and other veterinarians about dermatology and has several publications in the field of dermatology and clinical microbiology. When she is not at VSH, she enjoys spending time with her retired racing Greyhound turned couch potato named Jack, and her very huggable and cuddly rescued Pit bull named Hadley.