Ruth Marrion, DVM, PhD, DACVO
Bulger Veterinary Hospital, North Andover, MA
Glaucoma is among the most frustrating ocular conditions for both veterinarians and owners. In this article I hope to give some practical guidelines for diagnosis, treatment, and possibly the most important aspect of managing cases of glaucoma – owner counseling! Although glaucoma occurs in our feline patients it is much more common in dogs than cats, so the main focus here is canine glaucoma.
Diagnosis
Glaucoma presents as a red, painful, or cloudy eye. Dry eye, corneal ulceration, glaucoma and conjunctivitis appear similarly. I recommend a complete eye exam for any pet presented for a red, painful eye. This includes menace response, pupillary light response, Schirmer tear test, fluorescein stain and tonometry. If you find that a pet has one condition, complete the eye exam! Just because a dog has dry eye does not mean that she does not have glaucoma.
The only way to diagnose glaucoma is to measure intraocular pressure; either a Tonopen, TonoVet or a Schiotz tonometer is completely adequate for this purpose. The key to using any of these is experience and comfort with the instrument. I would encourage you to acquire one of these and to use it on a regular basis, on client animals as well as your own pets. Normal intraocular pressure is published as 10-25 mmHg. However this can vary with operator or tonometer differences. At my practice, a normal intraocular pressure range is more like 8-18 mmHg with either the TonoPen or the TonoVet. As you become comfortable with using your tonometer you will also find what is a normal intraocular pressure range in your hands.
Once you diagnose glaucoma, you will need to answer two questions in order to plan a course of treatment. The first is whether the glaucoma is acute or chronic, and the second is whether the glaucoma is primary or secondary.
Acute or chronic
Once you have concluded that a pet has glaucoma, it is important to determine whether the glaucoma is acute or chronic. Most chronic cases will be irreparably blind; eyes with acute glaucoma will be temporarily blind due to the effects of the increased intraocular pressure (IOP) on the optic nerve, and in some cases vision can return once IOP is normalized. Owner history may be helpful, but keep in mind that owners may understate the duration of the disease due to a lack of initial observation, or guilt at not seeking prompt veterinary attention.
Probably the most useful factor in determining chronicity is the size of the eye. Chronic glaucoma is the ONLY cause of enlargement of the globe (buphthalmos). In almost all cases, an enlarged globe is irreparably blind. There are a few exceptions to this rule – young animals, Cairn Terriers, Shar Peis, Australian Cattle Dogs and Chow Chows. The reason for this in puppies and kittens is thought to be the elasticity of the sclera. In the above-mentioned breeds, I do not know the reason why patients may retain vision in an enlarged eye, it is just a clinical observation of mine. However, if an adult animal of another breed has an enlarged globe, it is very likely that the eye is irreparably blind.
You may also perform a fundic examination to look for optic disk cupping, which indicates damage to the optic nerve from increased intraocular pressure. Compare the appearance of the optic disk to that of the contralateral eye, if the latter is healthy.
It is reasonable to try to restore vision in a pet with an eye that is not visibly enlarged, and in which the optic nerve is not apparently damaged. If you are confident that a glaucomatous eye is irreparably blind then you should consider a permanent solution to the glaucoma (see below).
Primary or secondary
The other question in evaluating a case of glaucoma is whether it is primary (hereditary) or secondary. Glaucoma is hereditary in numerous dog breeds, including Cocker Spaniels, Basset Hounds, Siberian Huskies and many others.
Causes of secondary glaucoma include lens luxation (common in Terrier breeds), uveitis, and intraocular tumors. A thorough ophthalmic examination should help in determining whether the case is primary or secondary. If the patient has a lens luxation, this condition limits the medications you may use (see below), and a lens extraction will likely be necessary for successful management of the condition. To determine if a pet has a lens luxation, perform an anterior segment examination. The peripheral lens (equator) of the lens should not be visible in a normal eye, if it is, the lens is luxated or subluxated (Fig. 1).
If a pet has uveitis concurrent with glaucoma, that condition will need to be addressed as well. Look for aqueous flare – take the small beam of a direct ophthalmoscope and shine the light into the anterior chamber, holding the ophthalmoscope 2-3 mm from the cornea. You will need to perform this test in a darkened room. If you see a hazy beam going through the (normally clear) anterior chamber, the pet has uveitis. Finally, a visible mass in an eye, or a darkly pigmented, thickened iris in a cat is suggestive of ocular neoplasia (Fig. 2).
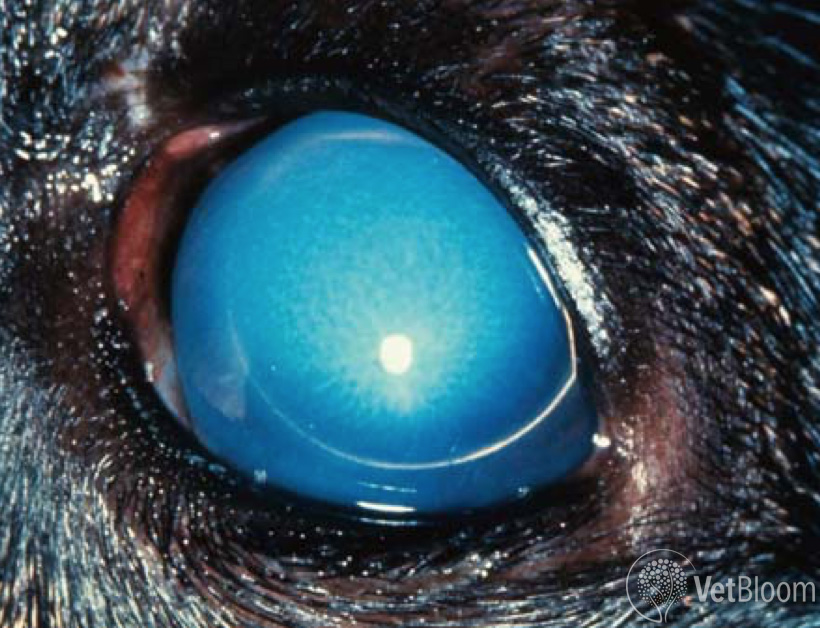 Fig. 1: Anterior lens luxation and secondary glaucoma in a terrier. Note that the lens equator is visible. |
 Fig. 2: Diffuse iris melanoma in a cat can cause secondary glaucoma. |
In some cases corneal edema will prevent visualization of the anterior chamber. In these cases signalment can suggest whether there is another condition (for example a young Terrier with glaucoma is likely to have an anterior lens luxation). In questionable cases you always have the option of referral.
Management of acute primary glaucoma
Glaucoma is increased intraocular pressure. We do not recognize a hypersecretory glaucoma in animals; therefore we can state that glaucoma is due to impaired outflow of aqueous humor. Whether treating medically or surgically there are two ways to address glaucoma: either improve outflow of aqueous humor, or decrease aqueous humor production.
Aqueous humor outflow occurs by two pathways in the eye, traditional outflow through the filtration angle, or uveoscleral outflow through the ciliary body. Traditional outflow is stimulated by the parasympathetic nervous system, acetylcholine endogenously, or a medication such as pilocarpine exogenously.
Uveoscleral outflow is stimulated by prostaglandins, so is responsible, at least in part, for the low intraocular pressure seen in uveitis. Prostaglandin analogs are molecules that have been chemically modified to maximize the hypotensive effects of prostaglandins while minimizing uveitis. These medications, however, typically cause profound miosis as well as mild inflammation (as evidenced by aqueous flare).
I have a protocol that I use in cases of glaucoma for which I think that there is some hope for restoration of vision. For dogs, I start with a drop of latanaprost (original trade name Xalatan), except in cases of lens luxation. (This medication does not work well in cats.) Latanaprost is a prostaglandin that has been modified to lower intraocular pressure dramatically, but also causes some signs of uveitis. In some dogs, latanaprost alone will be adequate to control intraocular pressure. If intraocular pressure does not normalize within an hour, I will add a topical carbonic anhydrase inhibitor such as dorzolamide (Trusopt) or brinzolamide (Azopt) TID, Pilocarpine 2% TID (except in cases of lens luxation), and timolol 0.5% BID. You also have the option to use mannitol for acute glaucoma cases. I tend not to use this medication only because it is cumbersome – one person needs to be dedicated to its administration over a 20-minute time period through an intravenous catheter. Furthermore there are potential dangers with mannitol use; noteably with cardiac or renal disease patients. However, mannitol can be an effective emergency treatment for glaucoma, so this can be part of the medical armamentarium to treat glaucoma if used cautiously.
Use both Pilocarpine 2% and timolol 0.5% with caution in cats and small dogs, as these can both cause bradycardia.
Most veterinary hospitals do not keep dorzolamide and latanaprost on hand since they will be infrequently needed except in a hospital with full time ophthalmology services. We generally send owners out to a 24 hour pharmacy to pick up these medications for in-hospital use. Both of these medications have become available as generic preparations in the past few years, and are much more cost-effective than are the brand name medications. For long term use, consider looking at the goodrx.com website. This provides information on the prices of medications of all kinds at different pharmacies.
If the above topical medications normalize intraocular pressure, I continue their administration. If they do not, I continue them and also I perform a passive aqueous centesis with a 27 or 30 gauge needle, to bring the intraocular pressure into the teens. (I understand that some practitioners may not be comfortable performing this procedure.) After normalizing intraocular pressure I continue all the above medications.
Once intraocular pressure is normalized, I recommend keeping the pet in the hospital to monitor pressure for 24 hours. There is no guarantee that IOP will not increase after this time, but I use 24 hours as a guideline. I tell owners that we can lower a dog’s intraocular pressure, but cannot guarantee that IOP will not increase again, or that vision will return. I emphasize to owners that the only measure that we can take to restore vision is to decrease IOP, and then wait to see if vision returns. If vision is going to return, it will do so within approximately two weeks.
I send dogs home with whatever treatment was necessary to normalize their pressures in the hospital. If latanaprost was adequate, I will send the dog home with this medication once to twice daily. If once daily, I recommend administering at night, since the profound miosis seen after administration can temporarily impair vision. Depending on the other medications I used in the hospital, I will send the patient home with topical timolol 0.5% BID and Trusopt TID. I will generally want to see the dog in a week, and then gradually decrease the frequency of recheck appointments as long as the dog is doing well.
I recommend treating the fellow eye of a glaucomatous eye with timolol BID long term. It has been shown that prophylactic treatment for a normotensive eye of a canine glaucoma patient will prolong the visual life of the eye by up to several years.
Management of acute glaucoma
- Latanaprost topically BID
- Dorzolamide topically TID
- +/- Pilocarpine 2% topically TID (contraindicated in pupillary block, caution in cats and small dogs
- +/- Timolol 0.5% topically BID (caution in cats and small dogs)
Management of acute secondary glaucoma
Lens Luxation – Anterior lens luxation physically blocks the pupil, disrupting the flow of aqueous humor from the posterior to the anterior chamber. This physical obstruction of the flow of aqueous humor is known as pupillary block glaucoma. Miotics (latanaprost, pilocarpine and other medications such as demecarium bromide) are CONTRAINDICATED in pupillary block glaucoma, since they exacerbate the obstruction to flow of aqueous humor out of the filtration angle at the junction of the cornea and sclera. I use tropicamide, which dilates the pupil without compromising the flow of aqueous humor out of the filtration angle. Glaucoma due to lens luxation is a surgical condition, and most of these dogs need lens extraction surgery to normalize intraocular pressure.
Uveitis – Pets with uveitis will need to be treated with a topical steroid such as prednisolone acetate, along with glaucoma medications. Some practitioners will avoid the use of latanaprost and other miotics such as pilocarpine in cases of uveitis. It is fine to start out with other classes of hypotensive medications initially, but if these do not work a miotic may need to be used in addition.
Tumors – Glaucoma secondary to an intraocular tumor is generally not going to respond well to medical treatment, and enucleation of the affected eye will likely be necessary.
Management of chronic glaucoma
Some cases of glaucoma in small animal patients do well with medical therapy long term. There are numerous surgical procedures for trying to maintain vision in eyes with glaucoma, and none has a high success rate, but surgery is a reasonable option for cases in which medical therapy does not control intraocular pressure. Veterinarians can feel free to contact me if they think a patient of theirs could benefit from a glaucoma surgery.
Once an eye is irreparably blind, I encourage owners to consider a permanent procedure to relieve the pain and discomfort of glaucoma. Enucleation (removal of the eye) and evisceration (placement of a prosthesis inside the cornea and sclera) are two options. These are major surgeries requiring general anesthesia. I usually perform intravitreal injections of gentamicin and triamcinolone to pharmacologically ablate the ciliary body. This procedure, which requires only a brief sedation, is based on the epitheliotoxicity of aminoglycosides. In the great majority of cases, one injection results in a permanent decrease in aqueous humor production and a comfortable, normotensive eye. The final appearance of the eye is variable – some are hyperemic, most develop cataracts, and some become phthisical. I tell owners that if they are unhappy with the appearance of the eye, they can always have it removed, and most of our clients are happy with the result. This procedure is ONLY indicated for canine eyes blind from primary glaucoma, since gentamicin also destroys the retina! Pharmacologic ablation of the ciliary body is contraindicated in cats, due to the risk of ocular sarcoma formation.
All too frequently dogs with glaucoma will lose sight in both eyes despite correct treatment. Many owners anthropomorphize and think that their blind dog will be miserable. They can be counseled to understand that blind dogs usually have a good quality of life. People often do not realize that dogs’ senses of smell and hearing are more important to them than their vision, and that blind dogs can generally memorize enough of their environment to get around well. There are several web sites and books available to give owners tips about dealing with a blind pet.
Two books we recommend for owners:
- Living with Blind Dogs: A Resource Book and Training Guide for the Owners of Blind and Low-Vision dogs by Caroline D. Levin
- Blind Devotion: Enhancing the Lives of Blind and Visually Impaired Dogs by Cathy Symons and Joan Powers