By: Beth Eisenberg, DVM, DACVECC
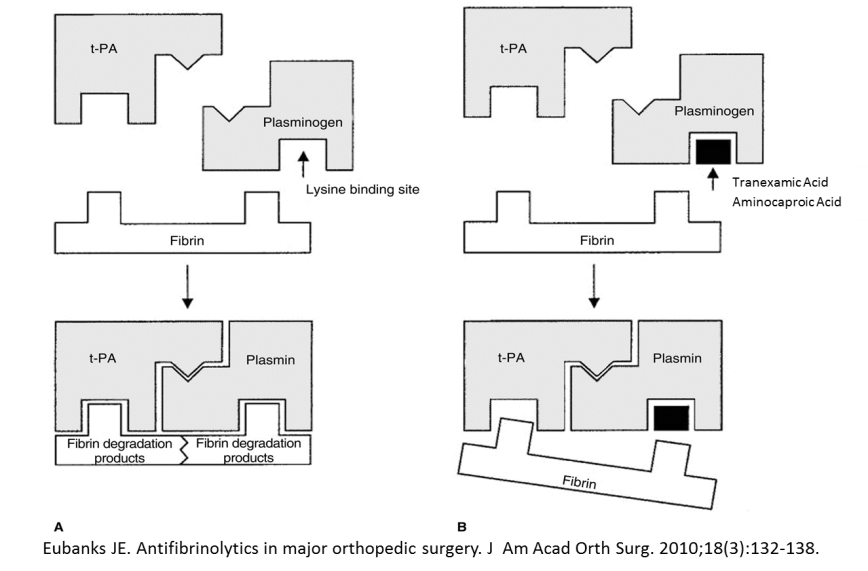
Epsilon aminocaproic acid (EACA) is an antifibrinolytic that can prevent excessive bleeding post-operatively, post-trauma, and in relationship to neoplasia. It is a synthetic lysine that targets the lysine binding site of plasminogen, preventing its binding to fibrin and conversion into plasmin (and therefore halts fibrinolysis). In humans a similar product called tranexamic acid has been shown to reduce bleeding episodes, all-cause mortality, and mortality due to bleeding in patients with severe trauma (CRASH-2 trial collaborators. Lancet 2010). There is growing evidence that EACA may also be helpful for patients with thrombocytopenic hemorrhage secondary to malignancy or chemotherapy (Kalmadi. Cancer 2006).
The documented uses in dogs are to prevent post-operative bleeding in greyhounds, who are known to have a higher than normal fibrinolytic activity. Use of EACA in these patients led to fewer and less severe bleeding episodes (Marin JVECC 2012, Marin Vet Surg 2012). A pilot study conducted at Michigan State showed that dogs with immune-mediated thrombocytopenia treated with intravenous EACA infusions had reduced hyperfibrinolysis (compared to placebo) and was well-tolerated (Ralph et al. IVECCS proceedings 2013). Dogs in liver failure have shown an increased incidence of hypocoaguability and hyperfibrinolysis on TEG tracings. This may explain clinically relevant post-liver biopsy bleeding in those patients that have normal PT/PTT levels (Webster C. ACVIM Proceedings 2014). An in-vitro study with injectable EACA given orally in dogs showed that the minimum dose required to improve clot strength and reduce fibrinolysis was 50 mg/kg (Brown et al. ACVS abstract). There is evidence that dogs likely require higher doses than humans to adequately reduce fibrinolysis (Fletcher AJVR 2014).
The recommended usage is as follows:
- For greyhounds undergoing surgery
- Oral EACA 500-1000mg PO per dog q8 hours, starting the night of surgery and continued for 5 days post-op OR
- 15-40 mg/kg IV immediately after surgery, then 500-1000mg total PO q8 for 5 days
- For dogs with acute hemorrhage suspected to be related to hyperfibrinolysis (severe trauma, uncontrolled bleeding with or without alterations in coagulation profile, thrombocytopenic hemorrhage)
- 50-100 mg/kg IV immediately, then 50 mg/kg PO q8 for 5 days
- Perioperative management of dogs with liver disease or dysfunction (not published)
- Oral EACA 500-1000mg per dog q8 hours, starting prior to the procedure and continued for 5 days after
- 50 mg/kg IV immediately after procedure, then 50 mg/kg PO q8 for 5 days
- For hemorrhage associated with thrombocytopenia (Abstract presentation IVECCs 2013)
- 30 mg/kg/hr for 2 hrs then 10 mg/kg/hr until platelets were ≥ 30,000/uL (Ralph 2013)
Information regarding injectable EACA formulation, pharmacodynamics, preparation, etc:
- At this time, any use of EACA in dogs is considered Off-Label. There are no reports regarding usage in cats.
- Dosage forms
- 20mL vial; 250 mg/ml
- Single-dose vial – unused portion should be discarded
- Store at room temperature
- Pharmacodynamics/kinetics (human information – no pharmacodynamics information exists for dogs)
- Renal excretion; severe renal impairment necessitates dose reduction due to markedly reduced clearance
- Water soluble
- Can be eliminated by hemodialysis
- Precautions/contraindications
- Rapid IV infusion may cause hypotension, bradycardia, or arrhythmia
- Safety in pregnancy is unknown
- Overdosage may result in acute renal failure, transient hypotension, and seizures. A lethal dose of 2.3g/kg has been reported in the dog.
- Can cause hyperkalemia in patients with renal impairment
- Oral formulation may cause GI upset
- Active intravascular clotting is an absolute contraindication (eg. DIC)
- Preparation and administration
- Add contents of 1 vial (20ml) to 230ml 0.9% NaCl to make a 20mg/ml solution
- Administer single dose IV over 30 minutes or as CRI
- Unused portion must be discarded
- The injectable formulation can be administered by mouth
References
- CRASH-2 trial collaborators. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomized, placebo-controlled trial. Lancet. 2010;376:23-32.
- Kalmadi S, et al. Epsilon aminocaproic acid reduces transfusion requirements in patients with thrombocytopenic hemorrhage. Cancer. 2006;107:136-140.
- Marin LM, et al. Retrospective evaluation of the effectiveness of epsilon aminocaproic acid for the prevention of postamputation bleeding in retired racing greyhounds with appendicular bone tumors: 46 cases (2003-2008.) J Vet Emerg Crit Care. 2012;22:332-340.
- Marin LM, et al. Epsilon aminocaproic acid for the prevention of delayed postoperative bleeding in retired racing greyhounds undergoing gonadectomy. Vet Surg. 2012;41:594-603.
- Ralph A, et al. A pilot study evaluating the safety and efficacy of aminocaproic acid for thrombocytopenic bleeding in dogs. Presented at IVECCS 2013.
- Webster CRL. To bleed or to clot: Management of hemostatic disorders in small animals with liver disease. ACVIM 2014 proceedings.
- Amicar package insert. Hospira 2015.
- Aminocaproic Acid Increases Clot Strength and Reduces Clot Lysis in an In Vitro Canine Model of Hyperfibrinolysis. Jamie C. Brown, Ben Brainard, Chad Schmiedt, Daniel Fletcher. ACVS Abstract.
- Fletcher DJ, et al. Evaluation of tranexamic acid and e-aminocaproic acids concentrations required to inhibit fibrinolysis in plasma of dogs and humans. Am J Vet Res. 2014;75:731-738.